
Vivinex™ iSert Toric IOL
 Spec Sheet
Spec Sheet


| Vivinex™ Toric |
| Model name | XY1A | |||
| Optic design | Biconvex with square, thin and textured optic edge: Anterior: Aspheric design | Posterior: Toric design | |||
| Optic & haptic materials | Hydrophobic acrylic Vivinex™ with UV- and blue light filter | |||
| Haptic design | Textured-rough haptic surface | |||
| Diameter (optic/OAL) | 6.00 mm/13.00 mm | |||
| Power | +10.00 to +30.00 D (in 0.50 D increments) | |||
| Cylinder power at IOL plane | 1.00 to 6.00 D (T2 to T9) T2 to T3 in 0.50 D increments T3 to T9 in 0.75 D increments | |||
| Nominal A-constant* | 118.9 | |||
| Optimized constants** | Haigis | a0 = -0.4362 | a1 = 0.2496 | a2 = 0.2035 |
| Hoffer Q | pACD = 5.682 | |||
| Holladay 1 | sf = 1.918 | |||
| SRK/T | A = 119.192 | |||
| Castrop | C = 0.323 | H = 0.1605 | R = 0.1193 | |
| Cooke K6 | A = 119.182 | |||
| Eom | A = 119.172 | |||
| Olsen | ACD = 4.84 | |||
| Injector | Vivinex™ iSert® preloaded | |||
| Front injector tip outer diameter | 1.70 mm | |||
| Recommended incision size | 2.20 mm | |||
| Model XY1A | Cylinder power at IOL plane | Cylinder power at corneal plane1 |
| T2 | 1.00 D | 0.69 D |
| T3 | 1.50 D | 1.04 D |
| T4 | 2.25 D | 1.56 D |
| T5 | 3.00 D | 2.08 D |
| T6 | 3.75 D | 2.60 D |
| T7 | 4.50 D | 3.12 D |
| T8 | 5.25 D | 3.64 D |
| T9 | 6.00 D | 4.17 D |
1Based on an average pseudophakic human eye.
*The A-constant is presented as a starting point for the lens power calculation. When calculating the exact lens power, it is recommended that calculations be performed individually, based on the equipment used and operating surgeon’s own experience.
**These optimized constants for the calculation of intraocular lens power published by IOLCon on their website: https://iolcon.org are calculated from clinical results for Vivinex™ Models XC1/XY1 and XC1-SP/XY1-SP as of November 10, 2025. These constants are based on actual surgical data and are provided by IOLCon as a starting point for individual constant optimizations. The information available on the website is based on data originating from other users and not by HOYA Surgical Optics (“HSO”). HSO therefore does not warrant the correctness, completeness and currentness of the contents on the said website.
Information contained is intended for health care professionals. For a full list of indications and contra indications please refer to the Instructions For Use. Some of the products and/or specific features as well as the procedures featured in this document may not be approved in your country and thus may not be available there. Please contact our regional representative regarding individual availability in your country. HOYA and Vivinex are trademarks of the HOYA Corporation or its affiliates. ©2024 HOYA Medical Singapore Pte. Ltd. All rights reserved.
1. Schartmueller, D. et al. (2019): True rotational stability of a single-piece hydrophobic intraocular lens. In: The British journal of ophthalmology 103 (2), p. 186–190.
2. Brar et al. (2024): Clinical outcomes and rotational stability following implantation of a monofocal toric IOL with textured haptics in normal versus high axial lengths. In: Journal of Cataract & Refractive Surgery, 50(7):p 718-723, July 2024.
3. HOYA data on file. CTM-23-027, HOYA Medical Singapore, Pte. Ltd, 2023.
4. Auffarth, G. U et al. (2023). Randomized multicenter trial to assess posterior capsule opacification and glistenings in two hydrophobic acrylic intraocular lenses. In: Scientific reports, 13 (1), 2822.
5. Tandogan, T. et al. (2021): In-vitro glistening formation in six different foldable hydrophobic intraocular lenses. In: BMC Ophthalmol 21, 126.
6. Perez-Merino, P.; Marcos, S. (2018): Effect of intraocular lens decentration on image quality tested in a custom model eye. In: Journal of cataract and refractive surgery 44 (7), p. 889–896.
7. Chandra et al. (2022): Effect of decentration on the quality of vision: comparison between aspheric balance curve design and posterior aspheric design intraocular lenses. Journal of cataract and refractive surgery 48 (5), p. 576-583.
8. Thakur, A. et al. (2024): Effect of decentration on the quality of vision in two aspheric posterior chamber intraocular lenses: A contralateral eye study. In: Indian J Ophthalmol. 72 (4), p. 558–564.
9. Leydolt, C. et al. (2020): Posterior capsule opacification with two hydrophobic acrylic intraocular lenses: 3-year results of a randomized trial. In: American journal of ophthalmology 217 (9), p. 224-231.
10. Giacinto, C. et al. (2019): Surface properties of commercially available hydrophobic acrylic intraocular lenses: Comparative study.In: Journal of cataract and refractive surgery 45 (9), p. 1330–1334.
11. Werner, L. et al. (2019): Evaluation of clarity characteristics in a new hydrophobic acrylic IOL in comparison to commercially available IOLs. In: Journal of cataract and refractive surgery 45 (10), p. 1490–1497.
12. Nanavaty, M. et al. (2019): Edge profile of commercially available square-edged intraocular lenses: Part 2. In: Journal of cataract and refractive surgery 45 (6), p. 847–853.
13. Matsushima, H. et al. (2006): Active oxygen processing for acrylic intraocular lenses to prevent posterior capsule opacification. In: Journal of cataract and refractive surgery 32 (6), p. 1035–1040.
14. Farukhi, A. et al. (2015): Evaluation of uveal and capsule biocompatibility of a single-piece hydrophobic acrylic intraocular lens with ultraviolet-ozone treatment on the posterior surface. In: Journal of cataract and refractive surgery 41 (5), p. 1081–1087.
15. Eldred, J. et al. (2019): An In Vitro Human Lens Capsular Bag Model Adopting a Graded Culture Regime to Assess Putative Impact of IOLs on PCO Formation. In: Investigative ophthalmology & visual science 60 (1), p. 113–122.
Our Vivinex™
Toric IOL
Proven benefits for you and your patients:
Clinically proven rotational stability. More than 96% of implanted lenses rotated ≤5° including eyes with high axial lengths1,2,3
Glistening-free hydrophobic acrylic IOL material 4,5
Incorporates the Vivinex proprietary aspheric optic design which partially compensates for corneal spherical aberration and is more tolerant to sources of coma than standard aspheric designs 6,7,8
Active oxygen processing treatment, a smooth surface, and square optic edge to reduce PCO4,9,10,11,12,13,14,15
*Third-party trademarks used herein are the property of their respective owners.
1. Schartmueller, D. et al. (2019): True rotational stability of a single-piece hydrophobic intraocular lens. In: The British journal of ophthalmology 103 (2), p. 186–190.
2. Schartmueller, D. et al. (2020): Comparison of Long-Term Rotational Stability of Three Commonly Implanted Intraocular Lenses. In American journal of ophthalmology 220, pp. 72–81.
Raising the bar
Maximum rotation values observed in the first week following surgery1,2
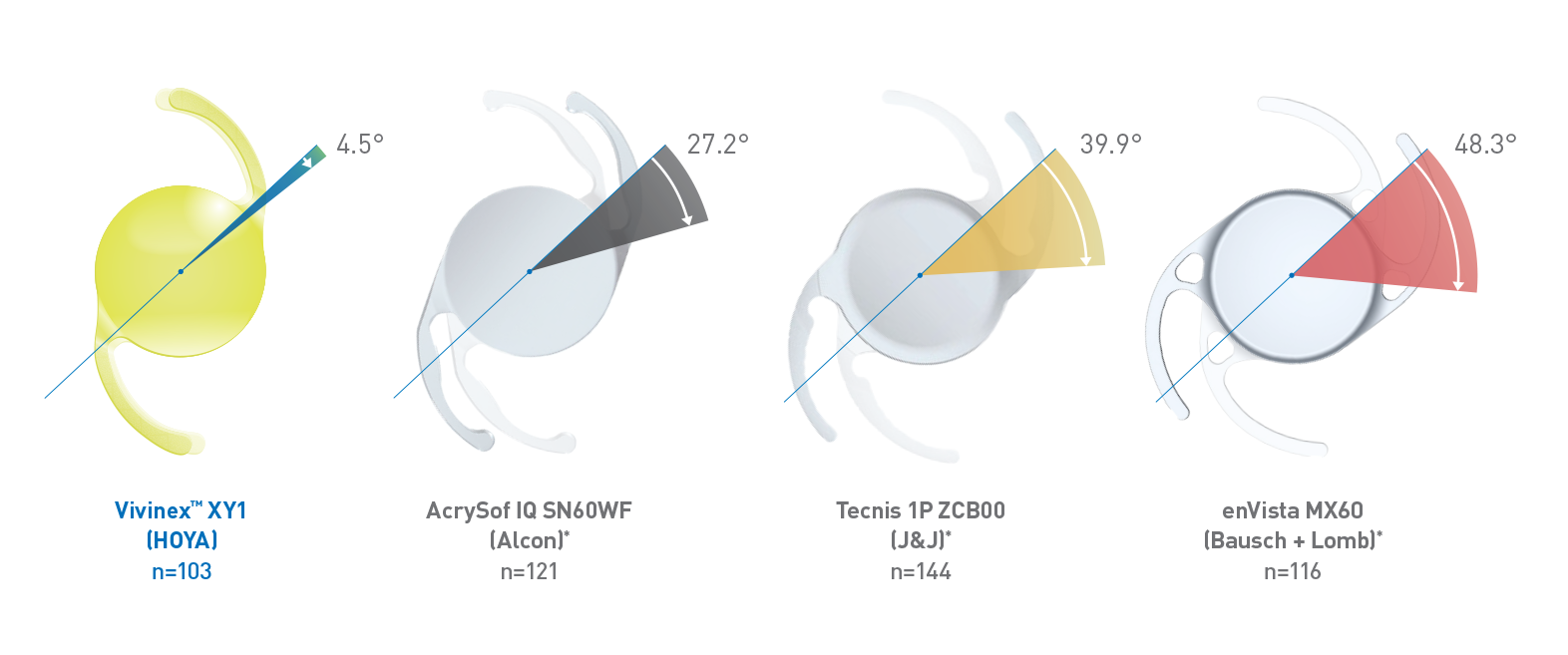
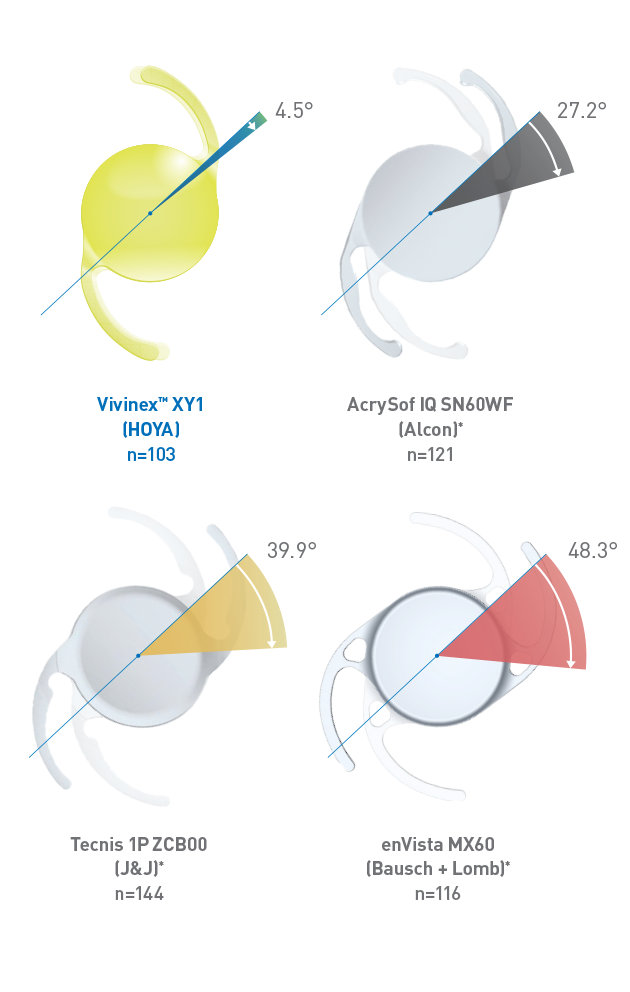
Reliable outcomes through outstanding rotational stability
The Vivinex™ IOL platform shows outstanding rotational stability between surgery and one week post op, without outliders, when compared with AcrySof®*, Tecnis®*, and enVista®*.1,2
*Third-party trademarks used herein are the property of their respective owners.
- HOYA data on file. CTM-23-027, HOYA Medical Singapore, Pte. Ltd, 2023.
Setting the standard for rotational stability
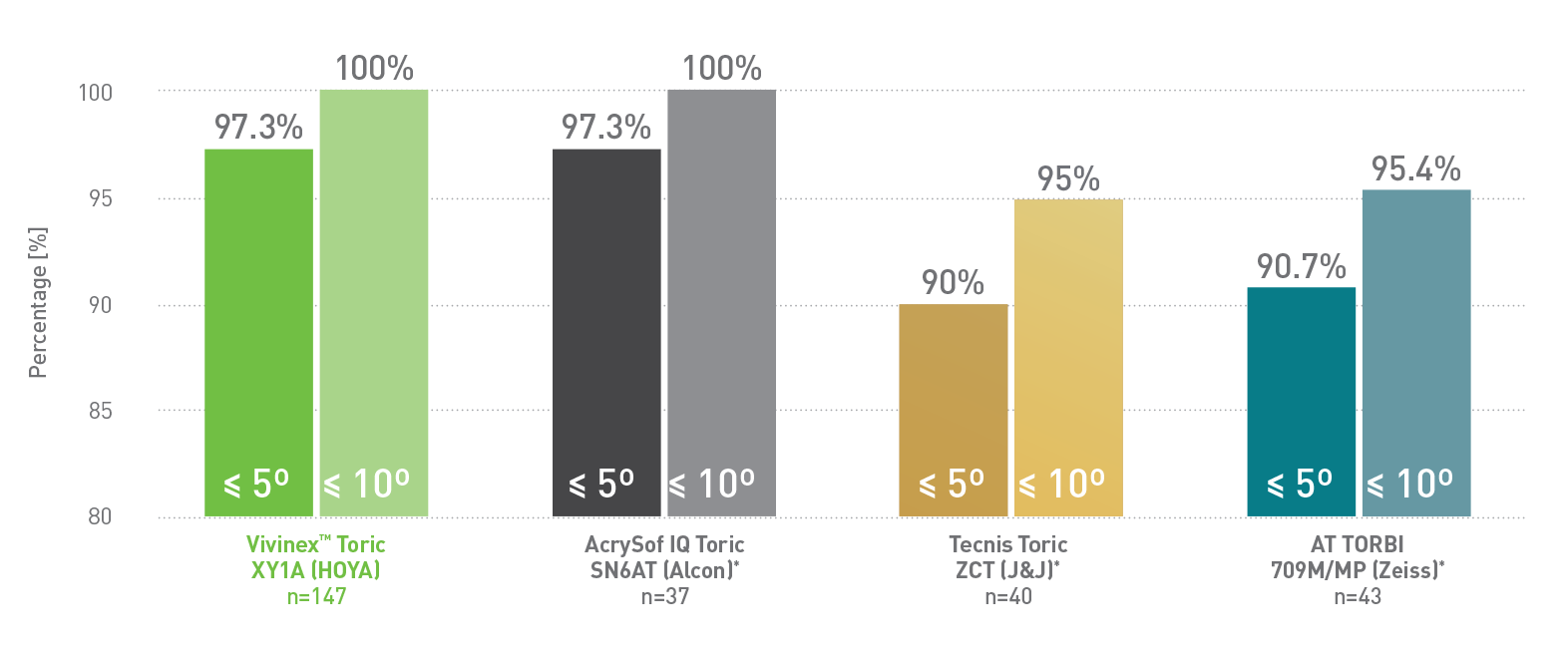
Distribution of absolute rotation between end of surgery and 6 months postoperative.
100% of VivinexTM Toric IOLs had less than 10° of rotation between the end of surgery and 6 months postoperatively.1
*Third-party trademarks used herein are the property of their respective owners.
1. Tandogan, T. et al. (2021): In-vitro glistening formation in six different foldable hydrophobic intraocular lenses. In: BMC Ophthalmol 21, 126.
2. Miyata, A. et al. (2001): Clinical and experimental observation of glistening in acrylic intraocular lenses. In: Japanese journal of ophthalmology 45 (6), p. 564–569.
3. Werner, L. et al. (2019): Evaluation of clarity characteristics in a new hydrophobic acrylic IOL in comparison to commerc ially available IOLs. In: Journal of cataract and refractive surgery 45 (10), p. 1490–1497.
Glistening-free clarity
In vitro glistening formation at 14x magnification1
Proven glistening-free IOL material with Grade 0 based on Miyata et al.2 in laboratory testings.1,3
- Pérez-Merino P, Marcos S. Effect of intraocular lens decentration on image quality tested in a custom model eye. J Cataract Refract Surg. 2018;44(7):889-896.
More than meets the eye
Watch how Vivinex™ improves image quality and reduces coma compared with other traditional negative aspheric IOLs.1

1. Auffarth, G. U et al. (2023). Randomized multicenter trial to assess posterior capsule opacification and glistenings in two hydrophobic acrylic intraocular lenses. In: Scientific reports, 13 (1), 2822.
2. Leydolt, C. et al. (2020): Posterior capsule opacification with two hydrophobic acrylic intraocular lenses: 3-year results of a randomized trial. In: American journal of ophthalmology 217 (9), p. 224-231.
3. Giacinto, C. et al. (2019): Surface properties of commercially available hydrophobic acrylic intraocular lenses: Comparative study.In: Journal of cataract and refractive surgery 45 (9), p. 1330–1334.
4. Werner, L. et al. (2019): Evaluation of clarity characteristics in a new hydrophobic acrylic IOL in comparison to commercially available IOLs. In: Journal of cataract and refractive surgery 45 (10), p. 1490–1497.
5. Nanavaty, M. et al. (2019): Edge profile of commercially available square-edged intraocular lenses: Part 2. In: Journal of cataract and refractive surgery 45 (6), p. 847–853.
6. Matsushima, H. et al. (2006): Active oxygen processing for acrylic intraocular lenses to prevent posterior capsule opacification. In: Journal of cataract and refractive surgery 32 (6), p. 1035–1040.
7. Farukhi, A. et al. (2015): Evaluation of uveal and capsule biocompatibility of a single-piece hydrophobic acrylic intraocular lens with ultraviolet-ozone treatment on the posterior surface. In: Journal of cataract and refractive surgery 41 (5), p. 1081–1087.
8. Eldred, J. et al. (2019): An In Vitro Human Lens Capsular Bag Model Adopting a Graded Culture Regime to Assess Putative Impact of IOLs on PCO Formation. In: Investigative ophthalmology & visual science 60 (1), p. 113–122.
What features of an IOL limit PCO?
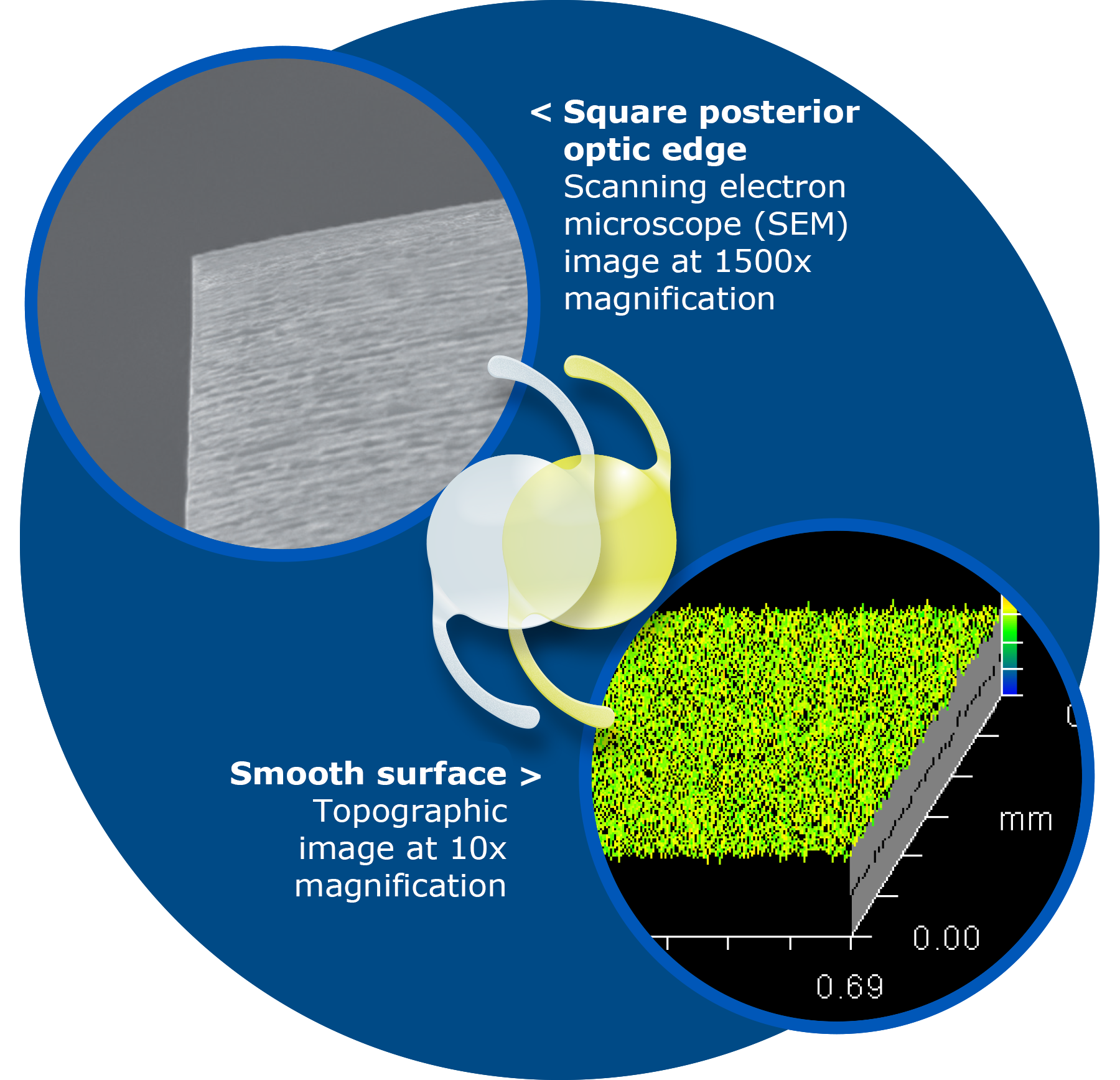
Vivinex™ combines an active oxygen processing treatment, a square edge design and one of the smoothest and most regular IOL surfaces to provide a low incidence of PCO.1,2,3,4,5,6,7,8
- Matsushima, H. et al. (2006): Active oxygen processing for acrylic intraocular lenses to prevent posterior capsule opacification. In: Journal of cataract and refractive surgery 32 (6), p. 1035–1040.
Want to learn more?
Watch how our active oxygen posterior surface treatment helps to reduce PCO.1
*Third-party trademarks used herein are the property of their respective owners.
1. Auffarth, G. U et al. (2023). Randomized multicenter trial to assess posterior capsule opacification and glistenings in two hydrophobic acrylic intraocular lenses. In: Scientific reports, 13 (1), 2822.
2. Leydolt, C. et al. (2020): Posterior capsule opacification with two hydrophobic acrylic intraocular lenses: 3-year results of a randomized trial. In: American journal of ophthalmology 217 (9), p. 224-231.
Are you interested in clinical proof?
| Vivinex™ XY1 (HOYA) | AcrySof® IQ SN60WF (Alcon) | ||||
|---|---|---|---|---|---|
| Objective (EPCO score) |
0.12 ± 0.19 | n = 57 | p < .026 | 0.24 ± 0.46 | n = 57 |
| Subjective (slit lamp score) |
0.30 ± 0.55 | n = 67 | p = .044 | 0.48 ± 0.84 | n = 67 |
| Nd:YAG rate | 0.0% | n = 67 | p = 1.00 | 1.5 % | n = 67 |
| Objective (AQUA score) |
0.9 ± 0.8 | n = 64 | P < .001 | 1.4 ± 1.1 | n = 62 |
| Subjective (slit lamp score) |
1.4 ± 1.4 | n = 64 | P = .001 | 2.3 ± 2.0 | n = 62 |
| Nd:YAG rate | 11.4% | n = 70 | p = .23 | 18.6 % | n = 70 |
In a randomized multi-center trial, Vivinex™ demonstrated significantly lower objective and subjective PCO scores compared with AcrySof® IQ after 3 years.1
In a randomized single-center trial, Vivinex™ demonstrated significantly lower objective and subjective PCO scores compared with AcrySof® IQ after 3 years.2
These results confirm low occurrence of PCO in both IOL groups and significantly lower PCO incidence with Vivinex™ compared to AcrySof® IQ.
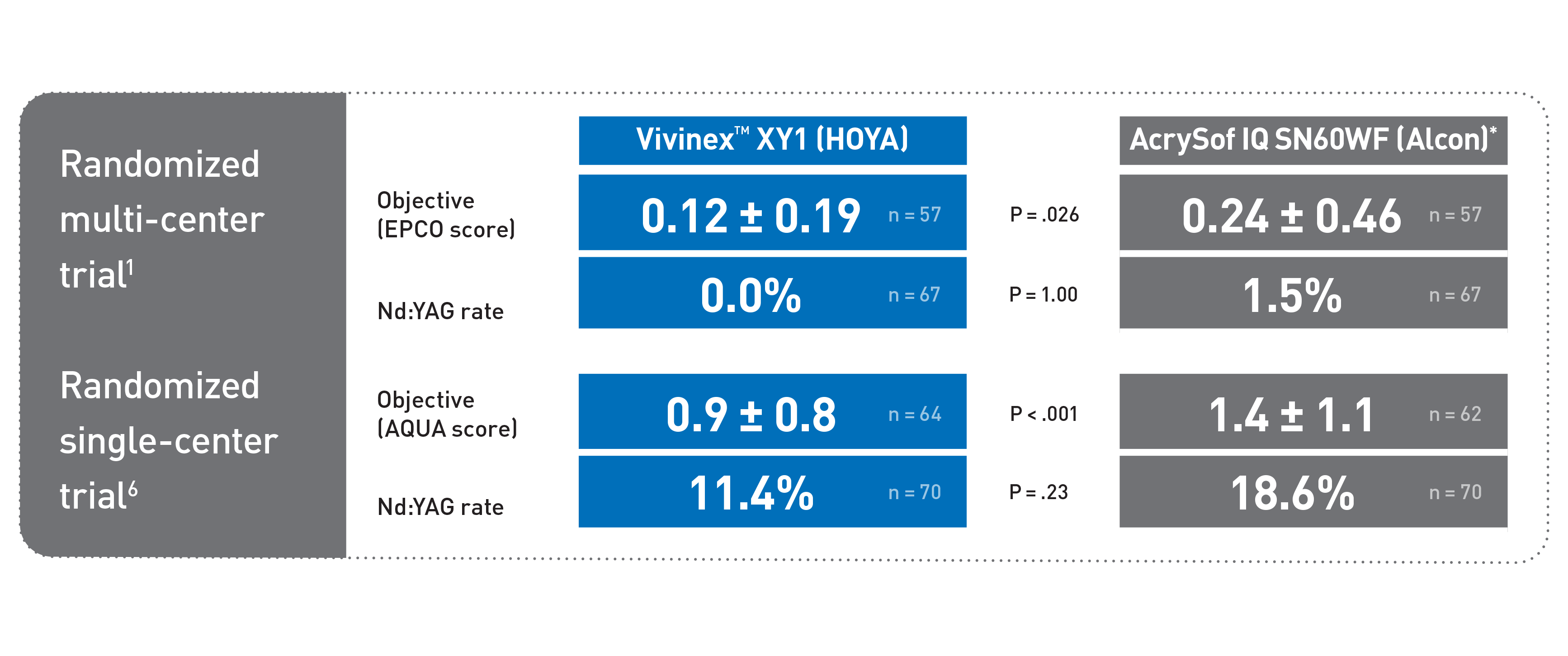
In a randomized multi-center trial and a randomized single-center trial, Vivinex™ demonstrated significantly lower PCO scores versus AcrySof* after 3-years. 1,2
Scroll